MI v/s HYPOGLYCEMIA
Long Case.
Hall ticket no - 1601006141
This is an online E-log book to discuss our patient's de-identified health data, after taking his/her/guardian's informed consent. Here we discuss our individual patient's problems through a series of inputs available global online community of experts with the aim to solve the patient's clinical problems with the collective current best evidence based inputs. This E-log book also reflects my patient centred online learning portfolio and your valuable inputs in the comments section.
My Case
Presentation.
A 70 year old gentleman, hailing from Nakrekal, a weaver by occupation was rushed to the ER (emergency room) at Kamineni institute of medical sciences Narketpally on 23/04/2021, following an episode of loss of consciousness for 1 minute on the same evening.
Emergency investigations and a quick history were taken;
Quick History:
- 2 episodes of giddiness since morning
- Giddiness was associated with
-sweating
-blurring of vision
-loss of consciousness for 1 minute
- no H/o
-decreased urine output, pedal oedema, facial puffiness
-involuntary movements
Investigations:
- GRBS- 2 mmol/L
- sPO2- 98% (at room atmosphere)
A decision was made to admit the patient to the hospital.
History.
Chief complaints.
- 2 episodes of giddiness one in the morning and the other in the evening associated with loss of consciousness for about 1 minute.
History of Presenting Illness.
- Patient was apparently asymptomatic till the morning of 23/04/2021, he then experienced 2 episodes of giddiness,sudden in onset, one in the morning and another as he pushed aside his table while weaving clothes at 4:00 pm. The giddiness was associated with loss of consciousness for which he was brought to the hospital.
- He had 3 more episodes of loss of consciousness at 10:00 pm on 23rd followed by another at 12:00 and another at 6:30 am. All of which occurred while he was in the hospital.
- The last syncopal attack lasted longer than the others and the patient suffered from post syncopal weakness in all 3 cases.
POSITIVE HISTORY.
- The giddiness was sudden in onset, associated with
profuse sweating
blurring of vision
palpitations
loss of consciousness (1 min)
[ patient says he remembers the moment upto loss of consciousness but cannot recall later events ]
[ He experienced post syncopal generalised weakness ]
NEGATIVE HISTORY
- No H/o
Blackouts
Photophobia
Phono phobia
Involuntary movements
Weakness of limbs
Involuntary micturition
Froth from mouth
Tongue bite
Up rolling of eyes
- No H/o
Trauma
Lifting heavy weights
Seizures
Postural drop of BP
Sensory or motor deficits
Fever, neck rigidity, projectile vomiting
Ear pain, discharge, tinnitus
Past History.
- No history of any similar complaints in the past
- He is a known case of - HTN, DM type 2 since 10 and 15 years respectively.
- Not a known case of cerebrovascular accident, coronary artery disease, bronchial asthma, tuberculosis, epilepsy, thyroid disorders.
Drug History.
- Patient has been on oral hypoglycemics for his type 2 diabetes since 15 years : Glimperide OD
- For his hypertension he was on the following medication since 10 years : Telmisartan OD
- Since he is at high risk for cardiovascular disease he was put on : atrovastatin + aspirin 75mg

Family History.
- No significant family history.
- No other family members are known cases of HTN or DM.
Personal History.
- Diet - Mixed
- Apetite - Normal
- Sleep - Adequate
- Bowel and bladder movements - Regular
- Addictions - Occasionally consumes alcohol, does not smoke
- No known allergies
Examination.
[ Informed consent was taken from the patient. ]
General Examination.
- Patient is conscious, coherent and co-operative, sitting comfortably on the bed with legs hanging by the side of the bed.
- Is well oriented to time, place and person.
- Moderately built and moderately nourished.
- General examination findings were as follows:
Pallor - absent
Icterus - absent
Cyanosis - absent
Clubbing - absent
Koilonychia - absent
Lymphadenopathy - absent
Edema - absent
[ examination for edema over the medial malleoli of both legs ]
VITALS SIGNS were as follows:
- Patient is afebrile.
- Pulse rate - 84 beats per minute, regular, normal in volume and character, no radio-radial or radio-femoral delay.
- Respiration - 18 cycles per minute
- Blood Pressure - left arm - 140/80 mm of Hg ; right arm - 160/80 mm of Hg
Systemic Examination.
Cardiovascular system.
- INSPECTION - chest wall appears normal [ transverse diameter greater than antero-posterior ] JVP is normal not elevated.
- PALPATION - carotid pulse felt on both sides; apex beat felt at left 5th intercostal space medial to mid clavicular line.
- AUSCULTATION - S1 and S2 heard, no cardiac murmurs
[ auscultatory examination ]
[ carotid pulse ]
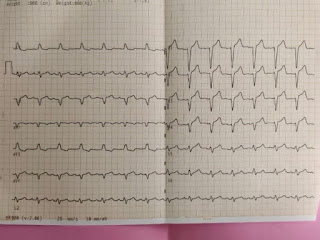
- Investigations done - ECG

[ electrocardiogram of the patient ]
Respiratory system.
- INSPECTION -
chest moves evenly with respiration
no intercostal retractions
no use of accessory muscles of respiration
trachea is central - no deviation
- PALPATION - inspection findings are confirmed
- AUSCULTATION -
normal vesicular breathing sounds are heard
bilateral air entry is present
no dyspnea/wheeze
- PERCUSSION - no abnormal dull notes heard, lungs are resonant.
Abdominal examination.
- INSPECTION -
all abdominal quadrants move evenly with respiration
no visible organomegaly
not distended
- PALPATION -
inspection findings are confirmed
liver is not enlarged non tender
spleen is not palpable
- AUSCULTATION -
no bruits heard
bowel sounds are normal
- PERCUSSION -
shifting dullness is not seen
liver span is normal
CNS examination.
- Patient is conscious, coherent and well oriented to time, place and person.
- No signs of meningeal irritation [ kernig's sign, brudzinki's neck and leg sign ]
- sensory system -
soft touch - normal
crude touch -normal
proprioception - normal
vibration sense - normal
- cranial nerves -
all cranial nerves function is maintained
- motor system -
power, tone, reflexes maintained in all limbs
PROVISIONAL DIAGNOSIS
ACUTE MYOCARDIAL INFARCTION DUE TO CORONARY ARTERY OCCLUSION CAUSING SUDDEN GIDDINESS AND LOSS OF CONSCIOUSNESS.
[ AS SUGGESTED BY HISTORY CLINICAL EVALUATION AND ECG FINDINGS SHOWING - ST SEGMENT ELEVATION ]
Investigations and treatment.
INVESTIGATIONS.
ECG
SERUM MARKERS
CORONARY ANGIOGRAM
ECHOCARDIOGRAM
CHEST X RAY
RADIONUCLIDE IMAGING [ IN HEMODYNAMICALLY STABLE PATIENTS ]
TREATMENT.
PRIMARILY MEDICAL TREATMENT INVOLVES THE FOLLOWING:
NASAL OXYGEN
GLYCERYL TRINITRATE SUBLINGUAL
IV HEPARIN
ASPIRIN, CLOPIDOGREL
BETA BLOCKERS ( METOPROLOL )*
ANALGESICS ( MORPHINE )
REPERFUSION THERAPY [ USEFUL IN ST ELEVATION MI ]
Reperfusion therapy is done in two ways :
percutaneous coronary intervention ( angioplasty/ stenting )
fibrinolysis ( streptokinase, urokinase, reteplase, tenecteplase )
Surgical treatment is coronary artery bypass grafting.

Comments
Post a Comment